Introduction
Choosing between open-heart surgery and a minimally invasive cardiac surgery approach can feel difficult, particularly when one option is described as having a smaller incision or faster recovery. The best approach, however, is not decided by scar size alone. It depends on the heart condition, the procedure required, the patient’s anatomy and overall health, the urgency of treatment, and the surgical team’s experience.
Open-heart surgery remains an important and established method for many complex operations. Minimally invasive techniques may offer meaningful benefits for selected patients, but they are not suitable for every case. This guide compares the approaches, explains eligibility and recovery, and outlines how patients can evaluate hospitals and surgeons responsibly.
Understanding the Two Approaches
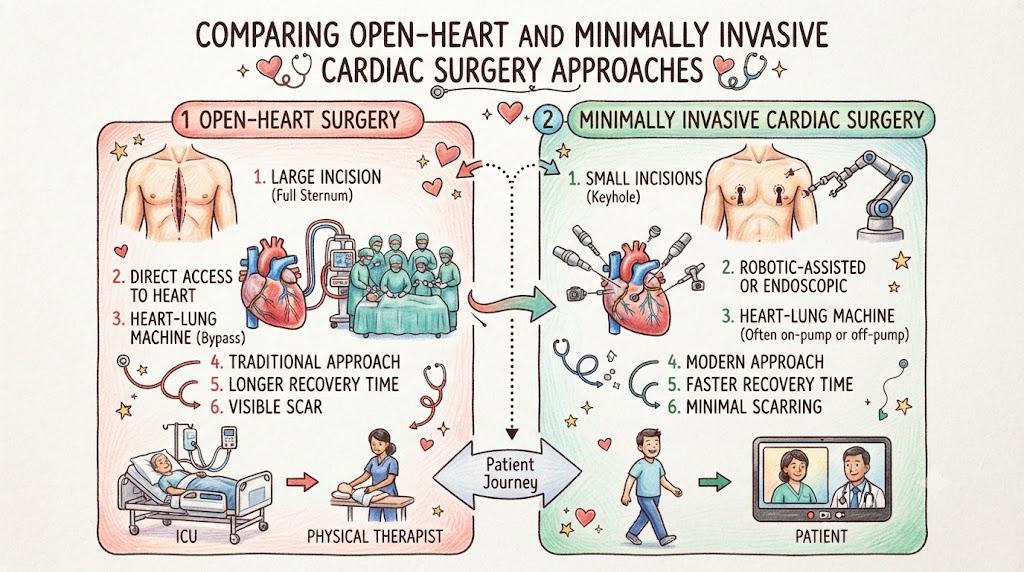
Open-heart surgery commonly involves a central chest incision and division of the breastbone, known as a median sternotomy. This gives the surgeon broad access to the heart and major blood vessels. Many operations use a heart-lung bypass machine, although the exact method depends on the procedure. The National Heart, Lung, and Blood Institute describes conventional open-heart surgery as involving a central chest incision, opening of the breastbone, and often cardiopulmonary bypass.
Minimally invasive cardiac surgery uses smaller chest incisions and may avoid dividing the entire breastbone. The surgeon may work through a small opening between the ribs, a partial sternotomy, thoracoscopic ports, or a robot-assisted system. Some minimally invasive operations still use a heart-lung machine. “Minimally invasive” mainly describes how the surgeon reaches the heart.
Patients should also separate minimally invasive surgery from transcatheter treatment. For example, transcatheter aortic valve replacement places a valve through a blood vessel rather than through a surgical chest incision. It is a different treatment category with separate eligibility requirements and risks.
Procedures That May Use Either Method
Selected heart valve repairs or replacements, limited coronary bypass operations, atrial septal defect closure, removal of certain cardiac tumors, and some rhythm procedures may be performed through smaller incisions.
Mitral valve surgery is one established area for minimally invasive and robot-assisted methods. The Society of Thoracic Surgeons describes mini-thoracotomy, direct-vision, video-assisted, and robotic approaches for selected mitral valve operations. Some aortic valve procedures can also use a partial sternotomy or small chest incision.
A full sternotomy may be preferred when several procedures are needed, coronary disease requires multiple bypass grafts, anatomy is difficult, surgery is urgent, or broad access is important. It may also be chosen when the team believes it offers the safest and most complete treatment.
Open-Heart and Minimally Invasive Surgery Compared
| Feature | Conventional Open-Heart Approach | Minimally Invasive Approach |
|---|---|---|
| Access | Central chest incision with full sternotomy | Small chest incision, partial sternotomy, or ports |
| Surgical view | Broad direct access | Focused access using direct vision, cameras, or robotic instruments |
| Common uses | Complex or combined procedures, multivessel bypass, emergencies | Selected valve, bypass, defect, or rhythm operations |
| Heart-lung machine | Commonly used | May still be used |
| Breastbone healing | Usually required | May be reduced or avoided |
| Recovery | Often longer because of sternum healing | May be quicker in suitable patients |
| Main limitation | Larger incision and longer restrictions | Not suitable for every patient or procedure |
| Conversion | Planned open access | May require conversion to sternotomy |
Potential Benefits of Minimally Invasive Surgery
For an appropriately selected patient, minimally invasive cardiac surgery may result in a smaller scar, less chest-wall disruption, lower postoperative pain, earlier mobility, and a shorter hospital stay. NHLBI notes that patients may have shorter recovery and lower pain levels after minimally invasive surgery, while emphasizing that it is not right for everyone.
Avoiding a full sternotomy may also reduce the period of breastbone-related activity restrictions. However, a small incision does not make the internal operation minor. The procedure may require specialized imaging, instruments, anesthesia, perfusion support, and a coordinated team. Benefits are possible rather than guaranteed.
Why Open-Heart Surgery May Be Preferred
Open-heart surgery provides wide exposure and allows the surgeon to reach several heart structures during the same operation. This is useful when the disease is complex, several valves or coronary arteries need treatment, or unexpected findings must be managed quickly.
A sternotomy can also provide flexibility in urgent cases. It is not an outdated method simply because the incision is larger. For many patients, it remains the safest way to perform a complete and durable operation. The key question is whether the proposed approach allows the surgeon to treat the heart problem accurately and safely.
How Suitability Is Assessed
The decision usually follows a detailed evaluation that may include an echocardiogram, coronary angiography, computed tomography, blood tests, and assessment of lung, kidney, and liver function.
Important factors include:
- The exact condition and its severity
- Whether one or several procedures are needed
- Previous chest or heart surgery
- Chest and blood-vessel anatomy
- Lung, kidney, and liver health
- Age, frailty, and mobility
- Infection or emergency status
- Need for complex reconstruction
- Surgeon and hospital experience
A patient may appear suitable at first but later be found to have anatomical or vascular factors that make small-incision surgery less safe. A minimally invasive operation may also be converted to sternotomy if visibility, bleeding control, or safe completion becomes difficult. Patients should discuss this possibility beforehand.
Risks and Complications
Both methods are major cardiac operations. Possible complications include bleeding, infection, abnormal heart rhythms, blood clots, stroke, kidney or lung problems, reactions to anesthesia, and the need for another procedure. NHLBI identifies arrhythmias, bleeding, clots, organ injury, and infection among recognized heart-surgery risks.
Risk depends on the patient’s condition, age, organ function, urgency, and procedure complexity. A smaller incision may reduce some wound-related concerns but does not remove the internal risks of operating on the heart.
Patients should request an individualized risk discussion. Some centers use validated surgical risk calculators to support shared decision-making, but these tools estimate probability rather than guarantee an outcome. The Society of Thoracic Surgeons provides procedure-specific risk tools for objective discussions between clinicians and patients.
Hospital Stay and Recovery
After either approach, patients are usually monitored in a cardiac intensive care unit before moving to a regular hospital room. Early care includes breathing support, pain control, wound care, walking, medication review, and monitoring for heart rhythm changes.
After sternotomy, the breastbone needs time to heal, and temporary limits may apply to lifting, pushing, pulling, and driving. NHLBI notes that complete recovery after conventional coronary bypass surgery may take approximately 6 to 12 weeks, while minimally invasive bypass patients often need less time.
Recovery after minimally invasive surgery may be faster, but patients should still expect fatigue and reduced stamina. Sleep, appetite, and mood changes can occur after either method. Follow-up testing and cardiac rehabilitation may be recommended. The American Heart Association states that valve-surgery recovery commonly takes several weeks and may be shorter after minimally invasive procedures.
Recovery Priorities After Cardiac Surgery
| Stage | Main Priorities | Useful Question |
|---|---|---|
| Intensive care | Breathing, circulation, pain, bleeding, and rhythm monitoring | When can tubes and lines be removed? |
| Hospital ward | Walking, eating, wound care, and medication adjustment | Which symptoms require urgent attention? |
| Early home recovery | Gradual activity, sleep, nutrition, and medicine adherence | What are my lifting and driving limits? |
| Follow-up | Review of healing, symptoms, heart function, and medicines | When can work, travel, and exercise resume? |
| Rehabilitation | Supervised exercise, education, and emotional support | Is cardiac rehabilitation appropriate? |
| Long-term care | Cardiology review and risk-factor control | Which tests and appointments are needed? |
Comparing Hospitals and Surgeons
A hospital offering robotic surgery is not automatically the best choice. Patients should compare the surgeon’s experience with the exact operation, the team’s procedure volume, cardiac anesthesia expertise, imaging and perfusion support, cardiac ICU staffing, infection-control systems, blood-bank access, emergency backup, rehabilitation, and follow-up care.
Patients may ask whether outcomes and complications are reviewed, who performs the main parts of the operation, and how concerns are handled after discharge.
International patients should clarify medical-record transfer, pre-arrival consultations, travel fitness, expected length of stay near the hospital, remote follow-up, medication supply, and emergency contacts after returning home.
The hospital should also be able to manage an unexpected conversion from a minimally invasive operation to an open procedure. Access to experienced cardiac anesthesiologists, perfusion specialists, critical-care teams, diagnostic imaging, and emergency blood services is therefore important.
Costs and Written Estimates
Costs vary according to procedure complexity, hospital category, city, room type, professional fees, diagnostic tests, operating-room time, ICU stay, implants, medicines, blood products, rehabilitation, and complications.
Minimally invasive surgery may require specialized instruments, robotic systems, advanced imaging, or longer operating-room time. This can increase the initial charge in some hospitals. A shorter hospital stay may offset part of that cost, but not in every case.
A written estimate should explain whether it includes:
- Cardiac surgeon and assistant surgeon fees
- Anesthesia and perfusion charges
- Preoperative diagnostic tests
- Operating-room charges and consumables
- Heart valves, grafts, or other implants
- Cardiac ICU and room charges
- Medicines and blood products
- Physiotherapy or cardiac rehabilitation
- Follow-up consultations
Patients should ask about possible additional charges if the operation is converted to open surgery, complications require extra treatment, or hospitalization becomes longer than originally estimated. No treatment estimate should be viewed as a guaranteed final amount.
Second Opinions and Shared Decisions
A second opinion can help when surgery is complex, different approaches have been suggested, or the patient is uncertain about the recommendation. The second specialist should review scans, angiograms, test reports, medical history, and the proposed surgical plan.
A second opinion does not always produce a different recommendation. It may confirm that sternotomy is the safest option, identify a minimally invasive alternative, or suggest a catheter-based treatment.
The final decision should reflect medical suitability, expected completeness of treatment, individual risks, patient priorities, and the experience of the treating center. Patients should understand why the recommended approach is suitable for their particular condition rather than choosing solely because one method sounds more advanced.
Questions to Ask Before Choosing a Hospital or Surgeon
- Why is this surgical approach recommended for my condition?
- Can the same repair be completed through both approaches?
- How often do you perform this exact procedure?
- Which surgeon will perform the main parts of the operation?
- What could require conversion to a full sternotomy?
- Which risks are most relevant to my health?
- What tests are required before surgery?
- What is included and excluded in the cost estimate?
- How long may the ICU stay, hospitalization, and recovery take?
- Is cardiac rehabilitation recommended?
- What follow-up support is available after discharge?
- Who should be contacted if urgent symptoms occur?
Frequently Asked Questions
1. Is minimally invasive cardiac surgery safer than open-heart surgery?
Not automatically. Safety depends on the patient’s condition, anatomy, procedure complexity, overall health, and the surgical team’s experience. A smaller incision does not eliminate major cardiac surgery risks.
2. Does minimally invasive surgery avoid the heart-lung machine?
Not always. Many small-incision valve and other cardiac operations still use cardiopulmonary bypass. The term mainly describes how the surgeon reaches the heart.
3. Can every heart valve operation use a small incision?
No. Suitability depends on the affected valve, the required repair or replacement, previous surgery, anatomy, calcium deposits, and other heart conditions.
4. Does a robot perform robotic heart surgery independently?
No. The surgeon controls the robotic instruments throughout the operation. The robotic system assists with visualization, movement, and access but does not make independent surgical decisions.
5. Can minimally invasive surgery change to open surgery?
Yes. Conversion may be needed when the team requires wider access, improved visibility, better bleeding control, or a safer way to complete the operation.
6. Which approach usually causes less pain?
Many appropriately selected patients experience less incision-related pain after minimally invasive surgery. However, pain levels differ, and effective pain management is important after either approach.
7. When can a patient return to work?
Timing depends on the procedure, healing progress, complications, and type of employment. Desk work may resume earlier than work involving lifting or physical activity. Individual clearance is required.
8. Can older adults undergo minimally invasive cardiac surgery?
Possibly. Age alone does not determine suitability. Frailty, kidney and lung function, blood-vessel anatomy, disease complexity, and expected benefit must also be considered.
9. Should robotic technology determine hospital choice?
No. Robotic technology is only one consideration. Surgeon experience, cardiac ICU support, emergency backup, safety systems, outcomes monitoring, and follow-up care are equally important.
10. Is a second opinion useful before cardiac surgery?
It can be valuable for major, complex, or non-emergency procedures, particularly when more than one surgical or catheter-based approach may be medically reasonable.
Key Takeaways
- A smaller incision does not automatically mean a safer or simpler heart operation.
- Open-heart surgery remains appropriate for many complex or combined procedures.
- Minimally invasive cardiac surgery may support less pain and faster recovery in selected patients.
- Anatomy, medical condition, procedure complexity, and surgical experience should guide the choice.
- Hospitals should be compared by procedure-specific expertise, cardiac ICU support, safety systems, and follow-up care.
- Written estimates should clearly state inclusions, exclusions, and possible additional costs.
- A qualified second opinion can support informed decision-making when treatment options are uncertain.
Conclusion
Open-heart and minimally invasive cardiac surgery serve different clinical needs. A minimally invasive approach may offer a smaller incision and shorter recovery for suitable patients, while sternotomy may provide the access and flexibility needed for complex treatment. Careful evaluation by an experienced cardiac surgeon, transparent discussion of risks and costs, and comparison of hospital capabilities can help patients make a decision based on their individual condition rather than on technology or scar size alone.